

By: Chuck Vollmer, Jobenomics Founder & President
6 August 2020
Is COVID-19 the Grim Reaper as generally believed, and is it time to take a more aggressive nationwide testing approach to suppress this resurgent virus for once and for all?
Jobenomics is a bipartisan national grassroots movement focused on getting people back to work and mass-producing startup businesses. Massive numbers of small and nonemployer firms are needed to replace shuttered enterprises and grow the U.S. economy that has been decimated by the COVID-19 pandemic.
Jobenomics happens to know a great deal about the coronavirus. As part of the Jobenomics-Aleph Diagnostics team (https://alephdiagnostics.com/), on 5 March 2020, this author hand-carried the world’s leading COVID-19 antibody rapid point-of-care test kit to the U.S. Centers for Disease Control and Prevention (CDC) headquarters in Atlanta and has been involved in combating this virus ever since.
Jobenomics also knows a lot about the U.S. economy, small business (the engine of the economy), startup businesses (the seed corn of the economy), and workforce development (the lifeblood of the economy). Today, the U.S. economy is on a sugar high due to a government infusion of ten trillion dollars ($9.97T allocated) to keep the U.S. economy afloat as we recover from the aftermath of a pandemically-induced financial crisis. This level of spending can not last indefinitely. If we cannot quickly suppress this virus and return people to work, a 1930s level Great Depression, replete with violent social upheaval, is just around the corner.
The politicization of COVID-19 has deepened an already divided country to the point of political gridlock and civil insurrection. The Administration is struggling to win a war on two-fronts—the pandemic and opposition politics. These dual fronts are undermining our nation’s ability to suppress the coronavirus and restore the livelihoods of working Americans. As stated by President Lincoln before the last civil war, “a house divided against itself cannot stand.”
COVID-19 is not the apocalyptic Grim Reaper, as generally believed. As of 1 August 2020, this global pandemic claimed approximately 700,000 lives or 0.01% of the world’s population. 1/100th of 1% is such an inconsequential percentage that it hardly seems to qualify as a “pandemic.”
The media would have us believe that COVID-19 has the destructive killing power of a level-5 hurricane when it barely deserves tropical storm status. Few people grasp the fact that previous pandemics were between 200-times to 1,300-times more lethal than this ersatz Grim Reaper. Here is a list of the deadliest pandemics: 30,000,000 HIV/AIDS deaths (1981-Present); 45,000,000 Spanish Flu deaths (1918-1919); 56,000,000 smallpox deaths (1520); and 200,000,000 Bubonic Plague deaths (1347-1351).
As of 1 August 2020, the U.S. COVID-19 death count reached 150,000 or 0.05% of the U.S. population—a relatively low mortality rate. While 150,000 fatalities equate to 3-times the amount of U.S. Vietnam War battle deaths, this death toll is only ¼ the number of annual deaths due to heart disease (647,457) and cancer (599,108). Every life is priceless, but a sound perspective is essential to proper decision-making.
Each year, three million Americans are killed or seriously injured in auto accidents. This statistic is much grimmer than the number of victims claimed by COVID-19 Grim Reaper but deemed acceptable to the way of American life. In the same manner, we need to agree to an “acceptable” balance of COVID lives lost relative to livelihoods destroyed by emotional, mental, and economic distress.
Other countries are suppressing the COVID-19 pandemic. If Americans unite, as we did post-911, we can move past this crisis in short order. To do so, Jobenomics recommends the following:
- The American public needs to focus on further reducing the death toll. The CDC’s provisional death count metric is the most important and most reliable in CDC’s arsenal of data. Additionally, the American public needs to discern and refute the plethora of politically-spun statistics.
- As many 180 million Americans could eventually be infected, but the majority will experience no or minor symptoms. Consequently, the overreported number of new cases is a misleading metric since the potential figure is likely to be ten times higher than currently reported. Americans should not be afraid of learning who is infected, who may be immune, and who is presently coronavirus free.
- The number of hospitalizations is equally misleading and often sensationalistic. With a few exceptions, hospitals have adequate facilities to cope with COVID patients and have the wherewithal to obtain additional resources as needed. Moreover, the medical community has achieved amazing results in treating COVID-19 victims and reducing the number of deaths.
- America’s most pressing challenge is to abandon its reactive mitigation strategy in favor of a more proactive suppression strategy that has proven successful in many other countries, like South Korea and Canada.
CDC’s Provisional COVID-19 Death Counts by Week
Source: CDC COVID-19 Death Data and Resources
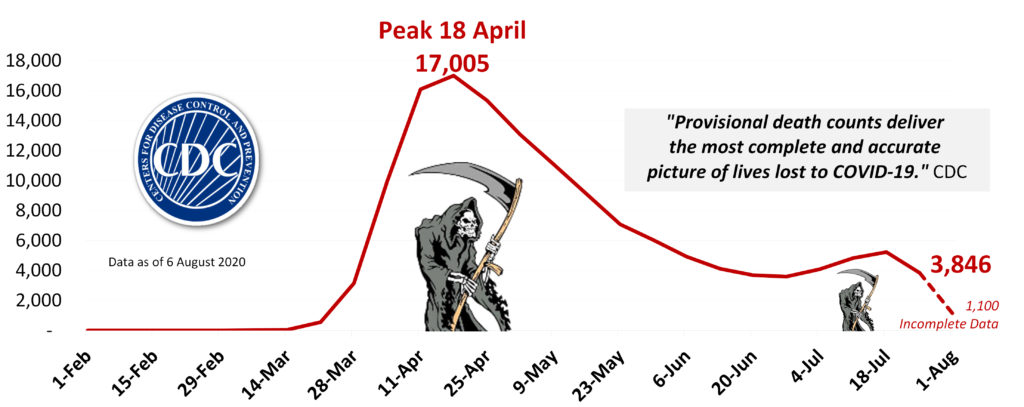
The attached 20-page report (free download) discusses each of these extensively researched and footnoted recommendations. The following graphic is representative of the many exhibits contained in the attached report, which provides the type of information you need to make informed decisions.
Contrary to what the national media wants the American public to believe, the COVID-19 Grim Reaper is a shadow of its former self (down from a peak of 17,005 fatalities per week in mid-April to 3,846 by the first week in August). While the United States reduced the Reaper’s killing power, we should keep vigilant. Hotspots, a second wave, and mutated viruses are likely.
From a grim reaper perspective, the vast majority of deaths claimed by this virus are older and elderly citizens, not the children or the working-age population.
- Older & Elderly Citizens (age 55+). This demographic consists of 94.7 million Americans or 29% of the population. If the “Grim Reaper” targets any specific age group, it is the older and elderly demographic that accounts for a colossal 92.1% of the deaths reported to the CDC.
- Prime Working-Age Citizens (age 25 to 54). This group consists of 128.6 million Americans or 39% of the population. Prime working-age adults represent only 7.7% of the deaths, many of whom have underlying medical conditions or low immune systems caused by genetics and poor lifestyles (smoking, drugs, obesity, etc.). Prime-age workers provide the goods and services necessary for a functioning economy. Without these critical workers, as well as the schools/daycare centers that allow working partners to return to work, our economy will not recover.
- Youth & Young Adult Deaths (age 24 and younger). This group consists of 103.2 million Americans or 39% of the population. COVID-19 deaths for individuals 24 years and younger amount to only 0.2% of the fatalities.
President Trump based his Fox News remark that children are “almost immune from this disease” using this CDC data. Only ten pre-school children (1-4 years) died out of a total of 142,164 people, or seven one-thousandth of 1%, which is pretty close to being immune. K-9th graders are only fourteen one-thousandth of 1% as likely to be a COVID-19 fatality. Based on these clinically reported facts, Facebook and Twitter were wrong to take down President Trump’s video. Both organizations claimed that the President’s remark violated their policies on coronavirus-related misinformation. Since Facebook and Twitter have not substantiated their claims, it appears that their actions were politically motivated.
Many other mainstream media outlets have joined the misinformation fray regarding the COVID-19 risk to children, especially as it relates to reopening schools. Headlines regarding the need to close daycare centers (21 million children), schools (57 million students), and universities (20 million undergrads) tend to more about the election than our children and their teachers.
Youth deaths due to influenza are 2½ times higher than COVID deaths. So why are we so inclined to shutter schools for COVID but keep them open during flu season? If a student comes down with the flu in class, we don’t necessarily need to quarantine the entire school if COVID-19 point-of-care test kits are readily available and provide results in minutes.
As of 6 August 2020, CDC’s COVID provisional death count was 144,073. By 29 August, CDC forecasts that the weekly U.S. COVID-19 death count will range between 4,500 to 10,600, resulting in a total death toll between 175,000 to 190,000 fatalities. This prediction is the composite of 31 provided forecasts from leading medical and research. Researchers at the University of Washington’s Institute for Health Metrics and Evaluation predict a total death toll of 295,000 by 1 December—the third leading cause of U.S. deaths in 2020.
While each life is precious, the COVID Grim Reaper is likely to claim many more lives until the United States achieves herd immunity. Herd immunity occurs when a large portion of a community (the herd) becomes immune to a disease, making it less contagious.
There are two ways to generate COVID-19 herd immunity—vaccines and infection. Infectious disease experts at The Johns Hopkins University explain that about 70% of the population needs to be immune to this coronavirus before herd immunity can work.
While vaccines are currently on the horizon, they should not be considered the primary solution to ending this pandemic. According to Dr. Fauci, the White House infectious disease expert, the chances for a vaccine being highly effective are “not great,” but a 50% rate would be considered a win. From a Jobenomics-Abbot Genetics perspective, an integrated vaccination/suppression testing strategy seems to be the only viable solution at this point in the pandemic.
The U.S. approach to dealing with the COVID pandemic is essentially a mitigation strategy that is not working. Mitigation strategies focus on slowing down transmission but not necessarily stopping epidemic with the protection of vulnerable groups and reducing peak healthcare demand. Slowing the spread of the infection is generally achieved via testing of mainly symptomatic cases, social distancing, mask-wearing, personal hygiene, and implementing stay-at-home quarantines. Had the coronavirus followed the seasonal path of its cousin, the influenza virus, mitigation might have been the proper U.S. strategy. Unfortunately, this virus is not seasonal, and outbreaks are frequent.
A suppression strategy involves a comprehensive approach to testing, contact tracing, and supported isolation (TTSI). Suppression-level TTSI programs help to reduce uncertainty fear, thus allowing people to feel freer to resume normal activities while still observing pandemic protocols, like mask-wearing. Suppression-level testing requires large-scale testing, including proactive testing of asymptomatic people (infected individuals who appear healthy) in vulnerable populations (e.g., the elderly) and high-risk environments (e.g., workplaces). The time to implement a proactive suppression strategy is now, before the advent of the flu season. There are plenty of state-of-the-art antibody, molecular, and antigen tests available now to start a nationwide effort.
The biggest obstacle holding back a nationwide suppression-level testing program is a national willingness to do so. We are a divided nation more interested in what separates us rather than our collective prosperity.
The second biggest obstacle is the preference for Made-in-America. While the FDA does not track foreign-produced pharmaceutics, experts estimate that 80% of the U.S. pharmaceutical drug supply comes from China. While Made-in-America is ideal for critical items, it is folly to believe we can accomplish this in a few months after decades of exporting our technology overseas.
Rather than trying to restrict Chinese-made pharmaceuticals, we should work with the Chinese to export their technology and create joint ventures to manufacture in the United States. This type of confidence-building effort is precisely what the Jobenomcs-Abbot Genetics team has negotiated with leading Chinese pharmaceutical companies for co-producing the Microfluidic Lab-on-a-Chip system in the United States.
Note: Download the entire 28-page “Is COVID-19 the Grim Reaper?” report to access source and footnoted data. Also, download other Jobenomics economic, community, small business, and workforce development efforts in the Jobenomics Library.

